
You line it up. You find the spot. Then the sensation flips.
What felt promising a second ago suddenly feels too bright, too sharp, too naked. You pull the toy away, or move your hand, or tense up without meaning to. Not because you’re not turned on. Because your body just went from interested to overwhelmed.
That experience is more common than people admit.
And it doesn’t mean your body is difficult, prudish, broken, or bad at pleasure. Most of the time, it means the signal got too concentrated, too exposed, or too fast for what your nervous system wanted in that moment.
“Too intense” doesn’t always mean the stimulation is objectively strong
This is the first distinction I’d make, because people mix these up constantly: intensity and pleasure are not the same thing.
A sensation can be powerful and great. A sensation can be powerful and immediately irritating. Same body. Same toy. Same general area. What changed is how the signal landed.
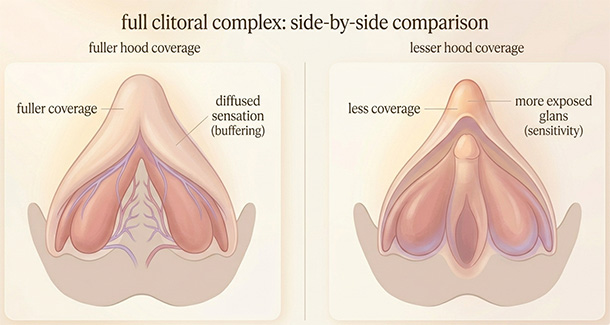
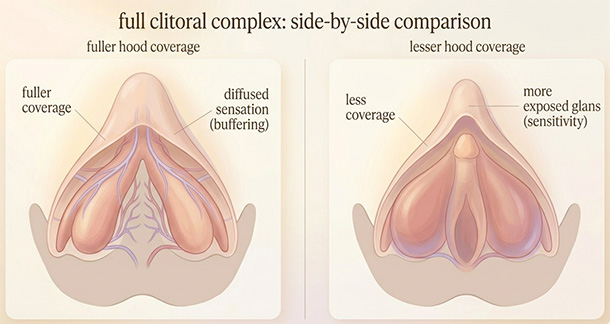
The visible glans of the clitoris is packed with nerve endings, and too much direct pressure there can hurt. The clitoris is also bigger than the tiny external nub people tend to picture. It’s a larger structure of nerves and erectile tissue, and the exposed part can be cushioned more or less depending on your anatomy, your arousal level, and what exactly is touching it.
That matters because “too intense” often has less to do with raw force and more to do with exposure. A light touch on highly exposed tissue can feel harsher than a stronger touch that lands through more buffer.
The spot may be right. The delivery isn’t.
That is often the whole difference between direct and indirect clitoral stimulation. Not a different pleasure center. Just a different amount of cushion between the contact and the most exposed tissue.
The same touch can suddenly cross the line because your body changed under it
This is the part people rarely get told, and it explains a huge amount.
Your body isn’t static while you’re turned on. Blood flow increases. Tissue swells. Lubrication changes. The clitoris becomes more sensitive as arousal builds, and for some people it can even become painful to touch directly once they’re highly aroused. In other words, the contact didn’t necessarily become worse. The body changed the conditions underneath it.
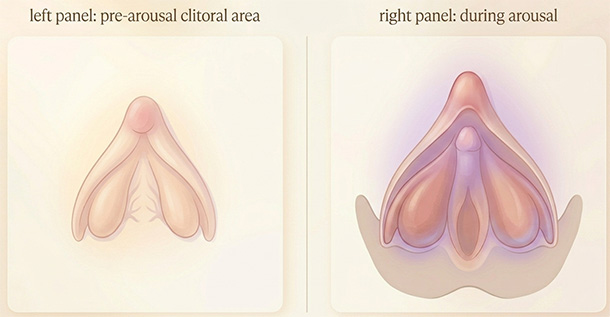
That’s why so many people say, “It was good until it wasn’t.”
They’re not changing their mind out of nowhere. The tissue got brighter, fuller, more responsive, and sometimes less tolerant of the exact contact that helped get them there in the first place. The same thing happens after orgasm, when one extra second of unchanged stimulation can feel almost rude.
And this is where the whole topic gets confusing: the clitoris is often both the route to orgasm and the first place overload shows up. The structure your body depends on most can also be the one that gets overwhelmed fastest. So yes, you can need steady clitoral stimulation to get there and still need that same stimulation to soften, shift, or back off at the finish line.
Pleasure can tip into sharpness before it tips into pain.
Sometimes the issue isn’t your sensitivity style. It’s the condition of the tissue
There are days when the problem isn’t technique at all.
Sometimes the tissue is dry. Sometimes it’s irritated. Sometimes hormone changes have made the area thinner, less resilient, or easier to aggravate. Sometimes the surface isn’t merely sensitive. It’s sore, inflamed, or reacting to friction before you even start properly.
Vaginal and vulvar dryness can bring soreness, itching, and discomfort during sex, and hormone changes, medicines, pregnancy, breastfeeding, menopause, and plain old low arousal can all play a part. Around menopause especially, vulvovaginal tissue can get thinner, drier, and less stretchy. That changes how touch lands. A toy that felt crisp and fun six months ago can suddenly feel scratchy or glaring.
This is where a lot of readers turn on themselves.
They think maybe they’re just too sensitive. Maybe they need to relax more. Maybe they need a softer toy, a stronger toy, better technique, a better mood, a different personality, apparently. But sometimes the more useful question is much simpler: is this tissue comfortable enough for touch today?
If the sensation feels raw, papery, burning, itchy, stingy, or sore even outside arousal, your body may be giving you a tissue clue, not a pleasure preference.
Pain conditions can hide inside what sounds like a preference
Some people really do prefer indirect touch. That’s normal.
Some people, though, are describing pain when they say they “just don’t like direct stimulation.” Those aren’t the same thing, and treating them like they are can keep people stuck for a long time.
Vulval pain conditions can feel burning, throbbing, stabbing, soreness, or pain triggered by touch, sex, tampon use, or sometimes by daily life itself. Nerve irritation, hormone changes, and pelvic floor issues can all be part of that picture. If the sensation goes electric, scraped, or instantly defensive within the first seconds, that can be a very different experience from simply wanting softer stimulation.
Those are not subtle differences once you know to look for them.
Preference usually sounds like, “I like this better over the hood,” or “I need more buffer first.” Pain often sounds like, “I touch it and my whole body says no immediately,” or “it stings even when I wasn’t trying to do much.” Readers can feel the difference in their bodies, but they often don’t have language for it, so everything gets filed under sensitivity.
Sometimes the body isn’t saying “less direct, please.” Sometimes it’s saying “something here hurts.”
The pelvic floor can make the whole area feel guarded
People often isolate the clitoris in their heads, like it’s one tiny switch with no neighborhood around it.
Bodies aren’t built that way.
When the pelvic floor muscles stay tight or guarded, they can contribute to pelvic pain and pain during or after sex. Pelvic floor dysfunction also shows up alongside orgasm difficulties often enough that it shouldn’t be treated like a fringe detail. If the surrounding system is already braced, even ordinary sensation can feel louder, sharper, and more threatening than it otherwise would.
So sometimes what you’re calling clitoral oversensitivity is actually a guarded pelvis. The contact isn’t only landing on sensitive tissue. It’s landing in a system that’s already halfway into defense mode.
That is often what people are feeling when body tension makes pleasure harder. The sensation doesn’t feel small. It feels unbuffered, amplified, and a little too close to alarm.
And because the pelvic floor and the clitoris aren’t separate little departments with their own HR policies, tension in one part can absolutely change how the other part feels.
What this usually looks like in real life
This is easier to understand in body language than in theory.
You’re using a suction toy. The first ten seconds feel promising. Then suddenly the sensation goes from building to glaring, and you yank it away before your brain has even put words to why.
You’re using your fingers. The pressure feels fine as long as it stays slightly off-center, but the second it lands more directly, your stomach tightens and the mood drops out of the room. Not forever. Just enough to make you annoyed.
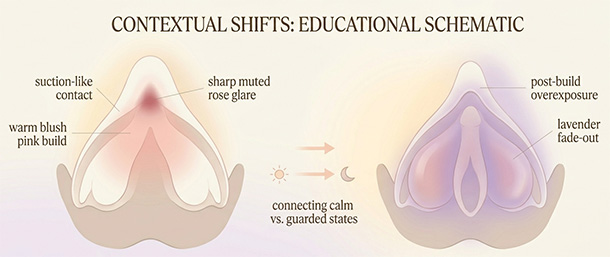
Sometimes you’re actually enjoying yourself, then you orgasm, keep the same contact for one beat too long, and the sensation becomes almost offensive. Not weak. Not numb. Just wildly overexposed.
On another day, the exact same toy feels terrible much earlier. Nothing obvious changed from the outside, but your body did: lubrication, cycle timing, stress, muscle tension, tissue comfort, arousal speed, all of it. That kind of whiplash is often what people are describing when the same toy can feel amazing one day and wrong the next.
For a lot of people, the next useful move isn’t less contact. It’s more buffer, which is often where to start when direct touch does not feel good. One layer up. Slightly off-center. Through the hood instead of straight on the glans. Same general area, different landing.
The nervous system doesn’t experience stimulation as one simple number. It experiences location, surface condition, pressure, timing, arousal state, and whether the rest of the pelvis feels open or defended. That’s messier, but it’s also why the body makes more sense once you stop trying to reduce everything to power level.
When to stop treating this like a technique problem
I would stop calling it “just sensitivity” and get it checked if the intensity comes with any of these:
- burning, stinging, itching, or soreness outside sexual touch
- pain with tampons, penetration, or even light contact
- symptoms that keep coming back, are getting worse, or are starting to affect daily comfort
- bleeding, unusual discharge, or ongoing dryness that is changing how the tissue feels day to day
That doesn’t automatically mean something serious is wrong.
It means the body may be asking for evaluation, not more endurance. A gynecologist, pelvic pain specialist, menopause-aware clinician, or pelvic floor physical therapist may help a lot more than another month of trying to out-technique a problem that’s no longer really about technique.
A better way to read the signal
I don’t read clitoral overstimulation as failure. I read it as precision.
Your body is telling you something specific about how sensation is arriving: too direct, too exposed, too fast, on tissue that is irritated, in a pelvis that’s bracing, on a day when the threshold is lower. That’s useful information. It gives you somewhere to work from.
Once you stop reading “too intense” as proof that you’re bad at pleasure, the whole thing changes. You stop trying to overpower the reaction. You start paying attention to what created it. Sometimes the answer is more buffer. Sometimes it’s less pressure. Sometimes it’s more arousal first. Sometimes it’s a medical issue that deserves actual care.
And sometimes it’s just one of those days when the body wants a little more distance before it says yes. That isn’t especially glamorous, but it is useful. Useful gets you further.
Reviewed medical and clinical sources
- Cleveland Clinic. Clitoris: Anatomy, Location, Purpose & Conditions. Cleveland Clinic. Medically reviewed; last updated January 26, 2026.
- Cleveland Clinic. Sexual Response Cycle: Order, Phases & What To Know. Cleveland Clinic. Medically reviewed; last updated December 27, 2023.
- Leicestershire Partnership NHS Trust. Female Orgasmic Difficulties. NHS patient information leaflet.
- Allison Conn, MD; Kelly R. Hodges, MD. Female Orgasmic Disorder. Merck Manual Professional Edition. Reviewed/revised July 2023.
- Allison Conn, MD; Kelly R. Hodges, MD. Sexual Interest/Arousal Disorder. Merck Manual Consumer Version. Reviewed/revised July 2023; modified January 2026.
- NHS. Vaginal Dryness. NHS. Page last reviewed July 24, 2025.
- NHS. Vulvodynia (vulval pain). NHS. Page last reviewed January 16, 2024.
- Cleveland Clinic. Hypertonic Pelvic Floor: Symptoms, Causes & Treatment. Cleveland Clinic. Medically reviewed; last updated April 26, 2022.
Add comment