
You go straight to the clitoris because that seems like the obvious answer. Then your body flinches.
Not because nothing is there. Because too much is there, too fast.
You move half a centimeter and suddenly it works.
That tiny shift throws a lot of people. They assume direct touch should feel better because it sounds more precise, more correct, more advanced somehow. But for many bodies, direct touch doesn’t feel better at all.
It feels exposed.
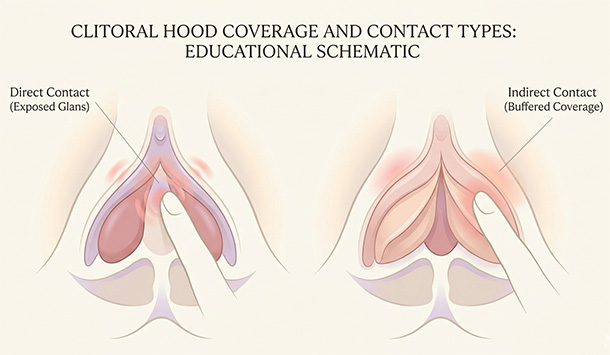
Direct and indirect are two distances from the same pleasure center
When people say direct clitoral stimulation, they usually mean contact right on the exposed glans. Indirect clitoral stimulation still stimulates the clitoris, just through something that softens the contact a little first: the hood, the tissue beside it, the mons, the inner labia, underwear, a blanket, the heel of your hand, the pressure of a body moving nearby.
That distinction matters because a lot of people hear “indirect” and assume it means vague, secondary, or somehow less real. It isn’t. The visible glans is only the outer part of a much larger structure, and the amount of hood coverage varies from person to person. So when you shift one layer up or one layer over and it suddenly feels better, you haven’t wandered onto the wrong organ. You’re still on the same system. The signal is just arriving with more cushion.
That small bit of buffering can change everything. For some people, it’s the difference between “absolutely not” and “keep going.”
Why indirect touch can feel better, even when the sensation is still clearly clitoral
The usual mistake here is assuming more direct means more effective. Bodies don’t work that neatly.
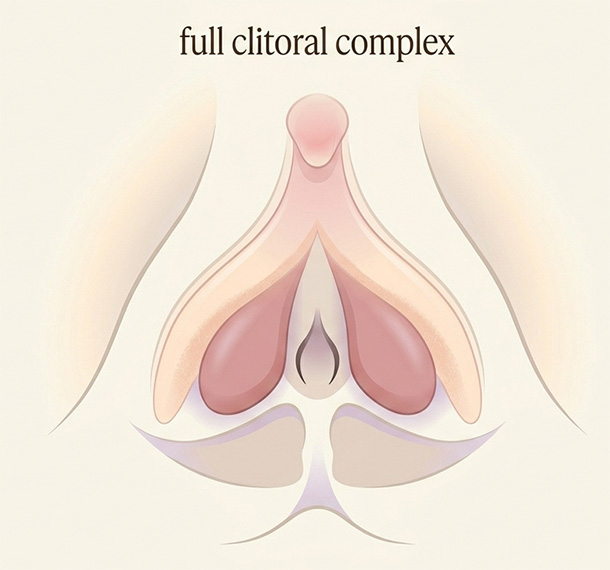
The clitoris extends inward. The surrounding tissue helps carry pressure, friction, and movement across that whole area. That’s why rubbing over the hood, the side of the glans, the tissue just above it, or around the vulva can still feel unmistakably clitoral rather than vague or accidental. The anatomy really does support that. This 2023 anatomy study mapped just how closely the clitoral body, vestibular bulbs, urethra, and nearby structures sit in relation to each other.
For some bodies, indirect touch doesn’t feel duller. It feels workable. The sensation is still focused and erotic, but it lands without that raw edge that makes you tense up before pleasure has a chance to organize itself.
That’s why filtered contact can be so useful. It often lands more like broad stimulation instead of pinpoint stimulation, and for a lot of people that broader, buffered feeling is exactly what makes the touch usable enough to build on.
You can feel the difference almost immediately. One kind of touch makes your body brace. The other makes it stay.
Why direct touch can feel better for some people, especially later
The buffer that feels perfect at one stage can start feeling like distance at another.
Once arousal is higher, some people want a cleaner line to the sensation. They want less softening, less tissue between the touch and the glans, less diffusion. Direct contact can feel easier to place, easier to repeat, and easier to build from once the body is ready for it.
And the variation here is completely normal. A large U.S. probability survey found wide differences not just in orgasm routes, but in preferred pressure, location, shape, and pattern of genital touch. That variation is the normal part. There is no final form your body is supposed to graduate into where direct touch becomes the superior, grown-up setting.
For one person, direct contact feels like finally getting to the point. For another, it feels like starting at volume 9 when the body was still trying to find volume 3.
That mismatch explains a lot of so-called sensitivity problems. The touch isn’t wrong in some abstract sense. It just lands so fast and so exposed that clitoral stimulation starts feeling too intense before pleasure has had room to gather.
Why intercourse confuses this question so badly
This is where people get misled by language.
They hear that penetration can stimulate the clitoris indirectly and assume that means penetration should be enough on its own. Sometimes it is. Often it isn’t. Many women need steady clitoral stimulation to orgasm, and penetration doesn’t reliably provide that by itself, which is one reason so many people end up feeling like they’re somehow doing sex wrong when really the mechanics just aren’t matching the body’s needs.
The numbers back that up. In that same large U.S. probability sample, only 18.4% of women said intercourse alone was enough for orgasm. Many said clitoral stimulation was necessary during intercourse, and many more said it made orgasm better. That shouldn’t be surprising, but decades of lazy sex advice have made it sound surprising anyway.
So when someone says, “I orgasm from sex,” the useful question usually isn’t whether penetration counts. It’s what else is happening. Are they rocking so the pubic bone stays in contact with the vulva? Is a hand involved? Is there oral stimulation before penetration? Is a toy doing some of the work? Are they thrusting, or are they grinding?
A 2021 nationally representative study gave names to some of those real-life adjustments. Women described rocking, where the base stays in contact with the clitoris, and pairing, where clitoral stimulation happens alongside penetration. That’s still clitoral pleasure. Penetration may be part of the scene, but the clitoris is often still doing the heavy lifting.
Your preference can change in the same session, which is where people start thinking they’re inconsistent
Early in arousal, direct touch can feel like too much information all at once. Later, once blood flow, engorgement, lubrication, and general arousal have built, that same contact may feel perfect. After orgasm, it may swing right back to being too much again.
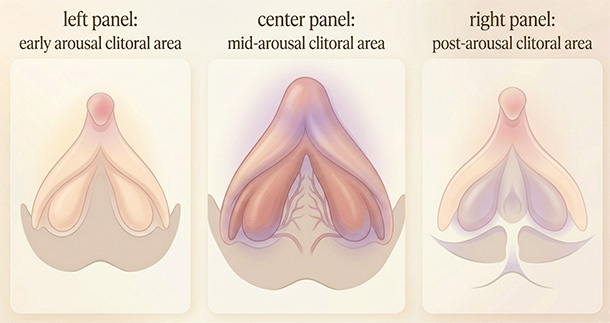
This is one reason people get confused by their own bodies. They think preference should stay stable from beginning to end, like you picked a setting and now the setting should behave. Bodies are less tidy than that. During arousal, the clitoris becomes more sensitive and may even become painful to touch directly. So the same contact can feel beautifully placed at one stage, then suddenly feel too sharp, too much, or weirdly wrong later.
That doesn’t mean your body changed its mind for no reason. It means the tissue changed, the arousal state changed, and the kind of input that feels usable changed with it.
It’s also why the same toy can feel amazing one day and wrong the next even when your technique looks identical from the outside. The body isn’t only reading pressure. It’s reading context.
What this actually looks like in real life
You touch the center of the clitoris with a fingertip and your stomach tightens immediately. Then you move that same finger one layer higher, over the hood, and the sensation stops feeling sharp. Nothing mystical happened. The pressure got buffered.
You put a vibrator directly on the glans and it feels like too much, too soon. Then you tilt it slightly to the side, or rest it above the clitoris instead of directly on top, and suddenly the sensation starts building instead of blasting. Same toy. Same body. Tiny change.
For some people, that small shift is the whole discovery. They don’t hate clitoral stimulation. They hate exposed clitoral stimulation. Through fabric, through the hood, through the heel of a hand, through the surrounding tissue, the same area becomes pleasurable enough to stay with.
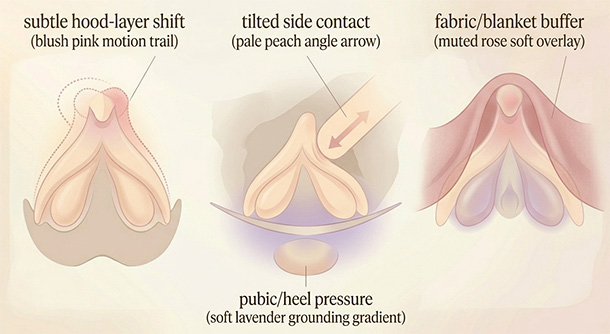
And this loops back to intercourse too. Sometimes you think penetration is what gets you there, but when you slow down and pay attention, the real driver is the pubic bone grinding against the vulva, or your hand reaching down at the right moment, or the base of the toy staying in contact instead of pumping in and out. That thread runs through the whole question. The clitoris keeps showing up, even when people use different words for the experience.
If direct touch doesn’t feel good, that’s often where to start when direct touch does not feel good: not with more effort, but with one layer more buffer.
A quick way to test what your body wants without turning it into a science fair
You don’t need a spreadsheet. You need one small comparison.
- Start one layer away from the center: over the hood, beside the glans, or with fabric between the touch and your skin.
- Keep the same rhythm longer than you want to. Too many people change too fast to read what their body is actually saying.
- If you pull away instantly, don’t add intensity. Add buffer.
- If it feels good but never gathers, reduce some of that buffer and get a little more precise. Not dramatically. Just enough to sharpen the signal.
The cleanest rule I know is this: if your body keeps bracing, go less direct. If your body keeps drifting, go a little more direct.
When this sounds less like preference and more like pain
There is a difference between “I like indirect better” and “this area burns, stings, aches, or hurts in ways that are bleeding into normal life.”
That difference matters.
If touch feels newly painful, pain shows up outside sexual moments, or sitting, walking, biking, clothing, soaps, or daily activity start setting it off, treat that as a medical issue worth checking rather than a preference note you need to optimize your way around. Clitorodynia can feel burning, stinging, throbbing, or aching. Vulvodynia can involve longer-lasting vulvar pain, sometimes provoked by touch and sometimes more diffuse.
If that sounds familiar, a gynecologist, pelvic pain specialist, or pelvic floor physical therapist is a better next step than more experimentation.
Pleasure preference is common. Persistent genital pain needs attention.
The better question isn’t which one is better
I wouldn’t ask which one is better in the abstract.
Better for what. Better when. Better in which phase of arousal. Better with what level of sensitivity, what kind of hood coverage, what kind of touch, what else your nervous system has going on that day.
Direct isn’t the gold-medal version of indirect, and indirect isn’t the beginner setting.
They’re two distances from the same pleasure center.
The useful question is simpler than that: which kind of touch does your body stop arguing with. Start there, and a lot of the confusion gets much quieter.
Reviewed medical and clinical sources
- Cleveland Clinic. Clitoris: Anatomy, Location, Purpose & Conditions. Cleveland Clinic. Last updated January 26, 2026.
- Tappy EE, Carrick KS, Ramirez DMO, Sawyer P, Corton MM. Anatomic relationships of the clitoral body, bulbs of the vestibule, and urethra. American Journal of Obstetrics and Gynecology. 2023.
- Mayo Clinic Staff. Anorgasmia in women – Symptoms and causes. Mayo Clinic. Updated February 29, 2024.
- Leicestershire Partnership NHS Trust, Department of Medical Psychology. Female orgasmic difficulties. NHS patient information leaflet.
- Herbenick D, Fu TCJ, Arter J, Sanders SA, Dodge B. Women’s Experiences With Genital Touching, Sexual Pleasure, and Orgasm: Results From a U.S. Probability Sample of Women Ages 18 to 94. Journal of Sex & Marital Therapy. 2018.
- Hensel DJ, von Hippel CD, Lapage CC, Perkins RH. Women’s techniques for making vaginal penetration more pleasurable: Results from a nationally representative study of adult women in the United States. PLOS One. 2021.
- Cleveland Clinic. Sexual Response Cycle: Order, Phases & What To Know. Cleveland Clinic. Last updated December 27, 2023.
- Cleveland Clinic. Clitoris Pain (Clitorodynia). Cleveland Clinic. Last updated July 18, 2022.
- Cleveland Clinic. Vulvodynia: Causes, Symptoms, Management & Treatment. Cleveland Clinic. Last updated December 27, 2022.
Add comment