
You keep drifting to one side.
Not by choice, exactly. More like your hand, your toy, or your hips keep correcting there because that is where the sensation starts to build instead of scatter. The other side is not numb. It just is not doing the same thing.
It doesn’t feel weaker. It feels less aligned.
If that’s your pattern, your body isn’t being weird. It’s being specific.
This is usually about contact geometry, not a broken side
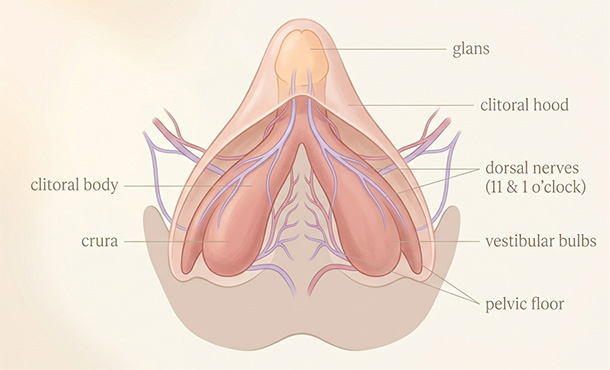
The first mistake people make is picturing the clitoris as one tiny, perfectly centered button that should respond the same from every direction. Bodies are rarely that symmetrical in practice. The visible glans is only one part of a larger structure. The hood may cover more or less of it. The surrounding folds are not always identical side to side. Even the inner lips can be symmetrical, asymmetrical, fuller, thinner, tucked, or more exposed.
That means a slight shift left or right is not a trivial change. It can move pressure from cushioned tissue to more exposed tissue. It can put the touch on a sheltered edge instead of a more direct, nerve-dense spot. It can also change whether the contact feels more like glans stimulation, hood stimulation, or pressure spreading into the structures packed around it.
A body can read those as different kinds of touch, not just slightly different versions of the same one. That’s often what people are really noticing when they compare direct and indirect clitoral stimulation and realize the angle changed more than the intensity did.
The clitoris is not a centered dot, and your favorite side usually proves it
The area is dense. That matters.
An anatomical study of the dorsal nerve of the clitoris found that the nerves course along the clitoral body around the 11 o’clock and 1 o’clock positions before entering the glans. A newer anatomy study described just how closely the clitoral body, vestibular bulbs, urethra, and nearby neurovascular structures sit to each other. In plain terms, slightly off-center touch can recruit different tissue and feel dramatically different.
This is why one side can feel more organized. One side catches in a useful way. The other catches in a distracting way. One gives your body something to follow. The other feels bright, thin, or too local to build on.
That difference matters more than people think. A sensation that gathers is easier to trust.
Sometimes one side simply has more cover, more buffer, or less drag
For some people, the “better” side is just the side with better cushioning.
Maybe that side has a little more hood coverage. Maybe the surrounding fold softens the friction there. Maybe the other side leaves the glans more exposed, so the same stroke that feels promising on one edge feels raw on the other. None of that is exotic. It’s just anatomy plus angle plus tissue.
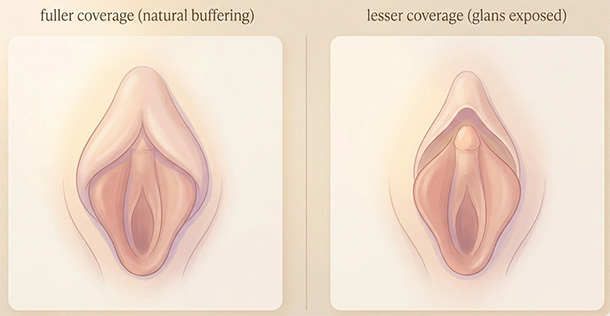
A millimeter can move you from buffered to unshielded.
And unshielded isn’t always sexy.
If one side suddenly starts feeling sore, itchy, pinchy, or oddly stuck, that deserves a different read. Structural issues around the hood, including adhesions, phimosis, debris, or keratin pearls, can cause localized discomfort. That is not the same thing as simple preference, even though people often file both under “I guess that side just feels bad.”
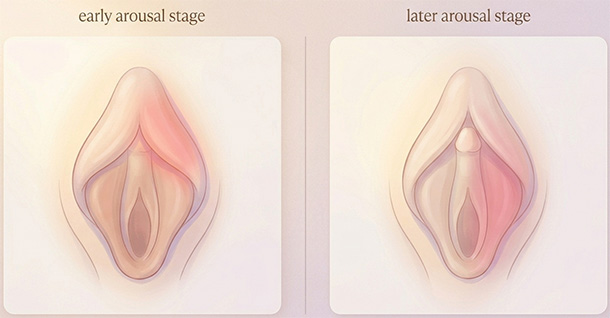
Your better side can change once arousal builds
This part surprises people because they expect sidedness to stay stable.
It often doesn’t.
A study in The Journal of Sexual Medicine found that clitoral vibratory sensation changed significantly between baseline and arousal. That lines up with what many people notice in real life. Early on, one side may feel vague while the other feels clean and usable. Later, once blood flow and sensitivity rise, the map shifts. The side that felt ideal at the beginning can become too direct. The side that felt almost absent can suddenly wake up.
So if you’ve ever thought, my body is inconsistent, that may not be the best explanation.
Your body may be consistent. You just checked it at two different stages. That is often the same reason clitoral stimulation can start feeling too intense even when nothing obvious changed from the outside.
What this looks like in actual use
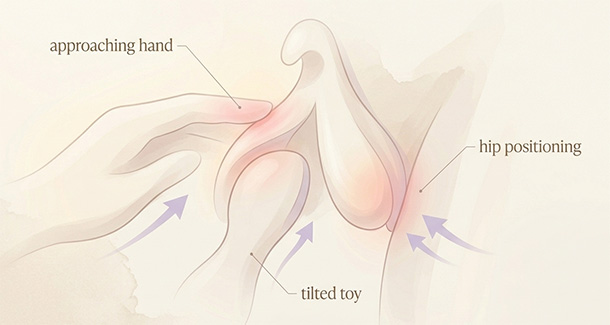
Usually, one-sided preference shows up in very ordinary ways:
- Your dominant hand approaches from one angle, so one side gets a smoother, more repeatable stroke.
- A toy head tilts slightly, and one edge ends up doing most of the work.
- One hip drops or one leg opens more, which changes how much of the glans is covered.
- Or a pillow, thigh squeeze, or grinding position shifts pressure just enough to wake one side up.
That is why people can swear a toy is too intense in one moment, then use the exact same toy five minutes later with a tiny angle change and suddenly understand it.
The body didn’t change that fast.
The contact did.
Sometimes what feels like a strong preference is really a repeatable geometry problem. One path across the tissue feels smooth and buildable. The other feels scratchier, brighter, or harder to stay with. Once you notice that, a lot of confusion clears up.
When one-sided sensation needs a medical look
Preference is one thing. Persistent one-sided pain is another.
If the same side is consistently burning, stabbing, itchy, numb, suddenly much less sensitive than before, or painful even with light touch, don’t brush that off as a quirky body. Vulvar pain can affect only part of the vulva, can be provoked by touch, and deserves evaluation if it keeps returning or doesn’t go away. Localized clitoral pain can also reflect structural or neuropathic causes.
Pelvic floor tension can matter here too. When the surrounding muscles are overactive, sexual touch can feel sharper, more defended, and less predictable. ACOG’s guidance on female sexual dysfunction notes that clinicians may use anatomy education and systematic touch mapping to localize symptoms more precisely.
That matters because “my clit hurts” and “the upper-right edge hurts when lightly touched” are not the same report.
And a good clinician can do more with the second one.
How to explore sidedness without turning it into a test
Do this once with curiosity, not as homework.
The minute it becomes pass-fail, most people stop noticing and start monitoring. That’s usually the point where exploring pleasure starts to feel like a test instead of actual exploration.
Start with enough lubrication or a barrier to reduce drag. Spend a short stretch on the left side of the hood or glans edge, then the same amount of time on the right. Keep the pressure and speed as similar as you can. Don’t chase orgasm. Just notice the quality of each side. Does one feel more buffered? More promising? Too exposed? Easier to stay with? Then check again later, once arousal has built, because the answer may change.
You are not trying to prove one side is correct.
You are learning what each side does.
That is a better question, and usually a more useful one.
The part most people miss
People are taught to treat symmetry as proof that a body is healthy. Equal on both sides. Equal every day. Equal in every position.
Pleasure doesn’t work like that.
Pleasure is directional. It is contextual. It is shaped by angle, cover, timing, tension, arousal, and the exact path touch takes across the body. Wanting one side more is not fussiness. It is not failure. It is not your body being badly designed.
A body that prefers one side is not difficult.
It’s articulate.
Reviewed medical and clinical sources
- Cleveland Clinic. Clitoris: Anatomy, Location, Purpose & Conditions. Cleveland Clinic.
- Cleveland Clinic. Vulva: Location, Anatomy, Function, Conditions & Care. Cleveland Clinic.
- Ginger VAT, Cold CJ, Yang CC. Surgical anatomy of the dorsal nerve of the clitoris. Neurourology and Urodynamics. 2011;30(3):412-416.
- Tappy EE, Carrick KS, Ramirez DMO, Sawyer P, Corton MM. Anatomic relationships of the clitoral body, bulbs of the vestibule, and urethra. American Journal of Obstetrics and Gynecology. 2023;228(6):720.e1-720.e8.
- Gruenwald I, Lowenstein L, Gartman I, Vardi Y. Physiological changes in female genital sensation during sexual stimulation. The Journal of Sexual Medicine. 2007;4(2):390-394.
- Krapf J, Pope R. Approach to Diagnosis and Management of Clitorodynia. O&G Open. 2025.
- NHS. Vulvodynia (vulval pain). National Health Service.
- Cleveland Clinic. Hypertonic Pelvic Floor: Symptoms, Causes & Treatment. Cleveland Clinic.
- American College of Obstetricians and Gynecologists. Female Sexual Dysfunction. ACOG Practice Bulletin No. 213.
- Mayo Clinic Staff. Female orgasm: No climax with vaginal penetration? Mayo Clinic.
Add comment