You keep adjusting the angle. A little higher. A little lighter. Then the sensation vanishes the second you think you’ve found it.
So you try to be more precise. Dead center. Slightly off-center. More pressure. Less pressure. Hood back. Hood down. After a while, the whole thing stops feeling like pleasure and starts feeling like you’re doing unpaid troubleshooting on your own nervous system.
That’s what bad advice does.
The old script says there’s one “right spot,” and if you aren’t getting results from it, you’re missing something obvious. I’ve hated that advice for years because it turns a three-dimensional organ into a dot and then quietly blames you when the dot theory fails. Plenty of people end up thinking their body is inconsistent, numb, too sensitive, or mysteriously difficult when the real problem is that the map they were handed was junk.
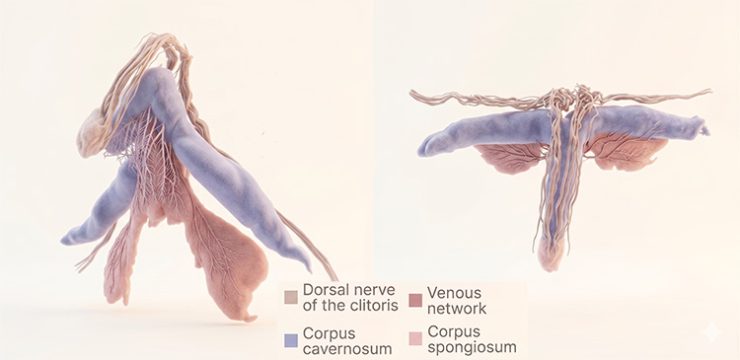
The new 2026 bioRxiv preprint on clitoral neuroanatomy doesn’t give us a magical orgasm coordinate. What it gives us is better anatomy. The researchers used very high-resolution 3D imaging on two postmortem pelvic specimens and traced the dorsal nerve of the clitoris in far more detail than routine dissection or standard imaging usually allows. Inside the glans, they found major nerve trunks branching toward the surface in a tree-like pattern. They also mapped branches reaching the clitoral hood and mons pubis, while the posterior labial nerve supplied tissue around the clitoral body and labia.
That matters because a tree isn’t experienced the way a target is. A target asks you to hit one point. A tree has a trunk, branches, smaller branches, spread, depth, and different surfaces catching contact in different ways. If your anatomy is organized more like that, then “just find the right spot” was never precise advice. It was oversimplified advice dressed up as precision.
That is also why direct and indirect clitoral stimulation can feel like two different conversations on the same body. The issue is often not whether the touch is technically “on the clitoris.” It is how much tissue is carrying the signal by the time it reaches you.
Older anatomy work and MRI studies had already been pushing back against the cartoon version for years. The clitoris is larger and more spatially complex than the visible external part suggests, and cadaver dissection work has shown that the clitoral body lies superficially under the hood and mons more than most people realize. The new paper doesn’t overturn that. It sharpens it.
And it gives people a much better reason to stop acting like failure to enjoy one tiny contact point means anything useful about your body.
Why the same area can feel sharp, blank, fuzzy, or suddenly perfect
Once you stop picturing a target and start picturing branching nerve pathways, a lot of confusing sensations make more sense.
Contact on the exposed glans can feel incredible for some people because it’s direct, concentrated, and clean. For other people it feels like too much signal hitting too little buffer. Not more intense in a good way. More like the sensation has nowhere to spread, so it turns thin and overbright. Then the same person tries through the hood, or slightly to one side, or with broader pressure that catches more tissue at once, and suddenly the body stops fighting the touch.
Broad contact doesn’t always feel weaker. Sometimes it feels like the sensation finally has somewhere to go.
That is the hidden reason broad stimulation works better than pinpoint contact. A wider landing area can turn a sensation that felt scratchy or overbright into one the body can actually build with.
That difference also fits with newer human innervation research. The 2024 Scientific Reports paper on the dorsal nerve of the clitoris found loose bundles rather than one neat cable and estimated denser innervation per surface area than in the penis. Dense sensory input can be wonderful. It can also mean your body notices tiny differences in angle, pressure, spread, and friction far more than lazy advice accounts for.
So yes, two millimeters can change everything. So can one layer of tissue. So can the difference between a fingertip and a flatter part of your finger. That isn’t you being fussy. It’s what a sensitive branching structure does.
And before somebody turns that into a new rigid rule, no, this doesn’t mean everyone should avoid direct touch or that the hood is always better. Some people love very direct contact. Some only like it after arousal has built. Some hate it almost every time. The point isn’t to replace one myth with a shinier myth. The point is to stop pretending there was ever one universal route.
The part bad advice gets really wrong is what it does to your head
The worst advice in this whole category is still “just find the right spot.” It sounds efficient. It isn’t. It trains you to override feedback from your body in favor of a script that keeps failing.
You stop noticing what feels promising and start auditing instead. Too high. Too low. Too direct. Too vague. You make a tiny correction, then another, then another, and by the time something almost starts to build, you’ve already interrupted it because you’re still looking for the approved answer. Pleasure turns into a debugging session.
Once that starts, it is very easy for the body to leave the sensation and start monitoring instead. That is exactly how performance pressure kills pleasure, even when the “performance” is happening alone in your own head.
I’ve seen people misread that process in brutal ways. They decide they’re low-sensitivity when the actual problem is that the touch is too pinpoint and scratchy. They decide they’re too sensitive when what they really need is more arousal before direct contact. They decide their body is inconsistent when the truth is more ordinary: the nervous system changes with context, hormones, stress, medication, sleep, dryness, pain, and whether the tissue is being contacted in a way that feels coherent or just noisy.
You’re not failing at something everyone else figured out at sixteen. The dominant script is wrong, and it’s been wrong in a very specific way.
What to actually try when “be more precise” keeps backfiring
This is the practical part, and it’s less glamorous than internet sex advice likes to be.
If you’re using fingers, start flatter than your instinct tells you. The pad of the finger usually works better than the tip, especially with enough lube that you’re gliding instead of dragging. A dragging motion can create friction that your brain reads as irritation long before it reads it as pleasure.
With a vibrator, I’d usually start lower than you think and stay there longer than feels productive. People sabotage themselves constantly by escalating before the tissue has even had time to organize the signal. What looked like a “weak” setting was sometimes the right setting that got abandoned too fast.
A few useful experiments:
- Try one pass with direct glans contact, then another through the hood without changing anything else. Not to prove which is superior. Just to hear the difference more clearly.
- Shift from pinpoint to broad contact on purpose. A smaller toy head or fingertip can feel exquisitely exact on some bodies and weirdly needly on others.
- Move less than you think. There are times when the upgrade isn’t a fancier motion but a steadier one that your body can actually build on.
- And if something starts working, stop “improving” it after ten seconds. A shocking amount of bad sex, solo and partnered, comes from people abandoning a good pattern because they think escalation is supposed to look busy.
Partnered sex has its own version of this problem. The biggest fix often isn’t a new trick. It’s keeping one effective pattern going for sixty seconds longer instead of switching the moment something starts to look promising. A lot of bodies need steadiness more than creativity.
If that line hits a nerve, it helps to think about whether your body builds better with steady pressure or constant movement. A surprising amount of near-miss pleasure disappears because the pattern changed before the nervous system had time to organize around it.
That thread from the opening comes back here. You weren’t necessarily missing the spot. You may have been interrupting the signal while trying to obey a bad map.
When the issue isn’t the map anymore
There’s another side to this, and it deserves a calmer voice.
Sometimes the problem really is technique, timing, or too much trust in terrible advice. Sometimes there’s a medical piece in the room and you shouldn’t have to keep guessing. If touch has started feeling newly wrong, it helps to separate a bad map from pain your body may actually be signaling. Burning, stinging, rawness, and persistent soreness are not the same problem as “I haven’t found the right technique yet.”
If you’ve developed new burning, stinging, rawness, pain with touch, sudden loss of sensation, or a sharp change after a medication switch, surgery, childbirth, or menopause, it’s worth talking to someone who knows vulvar and sexual pain instead of endlessly changing technique at home. ACOG’s vulvodynia guidance is very clear that burning, stinging, irritation, and touch-provoked pain are real symptoms, and newer clitorodynia guidance treats chronic clitoral pain as something that deserves actual evaluation.
The right clinician depends on the problem. A gynecologist with interest in sexual pain is a good start. A sexual medicine specialist is even better if you can find one. Pelvic floor physical therapy can matter when the surrounding muscles are part of the pain loop. You’re allowed to seek help before you’ve exhausted every DIY experiment on earth.
A better question to bring to your body
I’d retire “where’s the right spot?” for a while. It’s too small a question for what’s actually going on.
Try asking: what kind of contact is my body responding to here? That is a much more useful doorway into learning what kind of stimulation you actually like. Once you have language for the pattern — broader or narrower, steadier or more shifting, direct or buffered — your body usually starts sounding a lot less mysterious.
The tree metaphor helps because it gives you permission to stop acting like pleasure lives in one tiny bullseye. Branching anatomy means spread matters. Depth matters. Buffer matters. Timing matters. Some touch feels like a clean note. Some feels like static. Your job isn’t to be better at following bad instructions. It’s to notice which signal your nervous system can actually build with.
And when you find one, keep it there a little longer than your impatient brain wants to. That alone fixes more than people think.
Reviewed medical and clinical sources
- Lee JY, Alblas D, Szmul A, et al. Neuroanatomy of the clitoris. bioRxiv. Posted March 20, 2026. Preprint, not peer reviewed.
- O’Connell HE, Sanjeevan KV, Hutson JM. Anatomy of the clitoris. The Journal of Urology. 2005.
- O’Connell HE, DeLancey JOL. Clitoral anatomy in nulliparous, healthy, premenopausal volunteers using unenhanced magnetic resonance imaging. The Journal of Urology. 2005.
- Kelling JA, Erickson CR, Pin J, Pin PG. Anatomical Dissection of the Dorsal Nerve of the Clitoris. Aesthetic Surgery Journal. 2020.
- Tunçkol E, Heim C, Brunk I, et al. Innervation pattern and fiber counts of the human dorsal nerve of clitoris. Scientific Reports. 2024.
- Mayo Clinic Staff. Anorgasmia in women: Symptoms and causes. Mayo Clinic. Updated February 29, 2024.
- American College of Obstetricians and Gynecologists. Vulvodynia. ACOG Women’s Health FAQ.
- Krapf JM, Pope LE, Simon JA. Approach to Diagnosis and Management of Clitorodynia. Obstetrics & Gynecology. 2025.
Add comment