
You put your fingers where the internet said the spot was supposed to be. Instead of pleasure, you get one of three familiar disasters: too sharp, too vague, or weirdly nothing. So you start adjusting. A little higher. A little lighter. Smaller circles. Different angle. More lube. Then less. After a while, the whole thing starts feeling less like desire and more like customer support for your own genitals.
That can make you feel broken fast.
I don’t think that’s what’s happening.
One of the most persistent lies in sex advice is the idea that the clitoris is basically a little external switch. Find the exact point, stimulate it correctly, get the result. Clean. Efficient. Completely useless for a lot of real bodies.
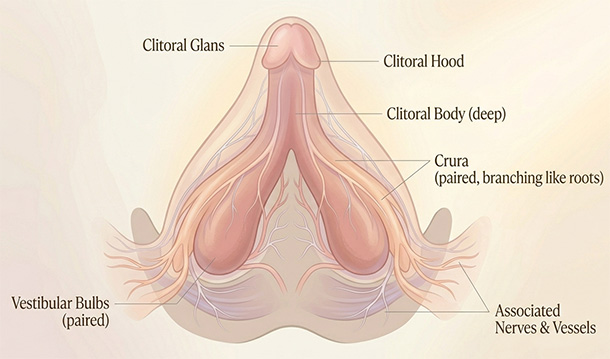
The visible glans is only the outer tip of a much larger internal structure, with erectile tissue and nerve-rich branches extending beneath the surface around the vulva. Once you understand that, a lot of otherwise confusing experiences stop looking mysterious. Of course some touch feels better when it’s broader. Of course one tiny point can feel too intense one day and strangely hard to track the next. You’re working with a network, not tapping a doorbell.
So when people tell you to “find the spot,” they’re already shrinking the body into something less interesting than it is. Good clitoral stimulation often works more like bringing an area online. The sensation needs room to gather. It needs contact your nervous system can keep reading without flinching or resetting every three seconds.
You’re not looking for one perfect pixel.
And for many people, orgasm depends on steady clitoral stimulation anyway, whether that comes from fingers, a toy, or indirect pressure through surrounding tissue. Penetration alone often doesn’t do the job. That isn’t a sign your body missed the memo. It’s the memo.
The first sign something is working usually isn’t fireworks
This is the part people skip past because they’re expecting pleasure to make a dramatic entrance.
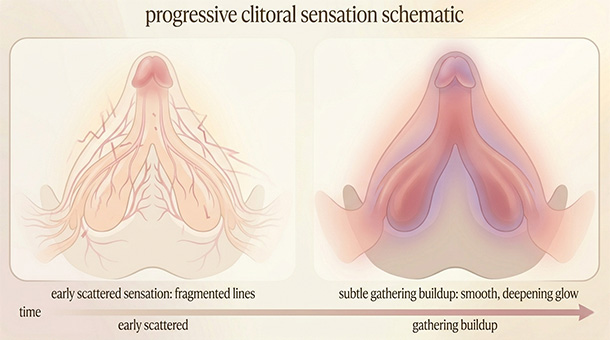
Sometimes it does. Often it doesn’t. Often the first useful sign is much quieter than that. The touch stops feeling thin. Your body stops shrinking away from it. The sensation starts to gather in one direction instead of scattering the second it lands.
You may not think, yes, that’s amazing. You may think, wait, don’t change that.
That’s a real shift.
The reason this matters is simple: if you think good stimulation has to feel intense right away, you’ll abandon working touch before it has time to become arousal. You’ll keep searching after your body has already started answering. And then you’ll walk away convinced nothing was happening, when what was happening just wasn’t loud yet.
For people who find direct contact too sharp, this is often the moment broader stimulation starts making more sense than pinpoint stimulation. The body isn’t asking for less pleasure. It’s asking for a signal it can actually stay with.
Later, that same contact can feel completely different. During arousal, the clitoris becomes more engorged and more sensitive, and touch that felt mild five minutes ago can suddenly feel like too much. That’s one reason the “just go harder” school of advice is so bad. Bodies change state. Good touch has to survive that change.
What pleasurable clitoral touch usually has in common
Bodies vary. Days vary. Stress, hormones, sleep, medication, dryness, distraction, and whether your brain is behaving like a menace all get a vote.
Still, touch that works well tends to share a few traits:
- It’s repeatable — your body can recognize it again on the next pass instead of decoding a brand-new signal each time.
- It feels sustainable. You aren’t bracing for impact or waiting for the sensation to turn annoying.
- There’s enough glide, softness, or buffering for the feeling to build instead of scrape across the surface.
- And it stays in place long enough to become something. People wreck this part constantly.
The usual failure point isn’t lack of effort. It’s interruption.
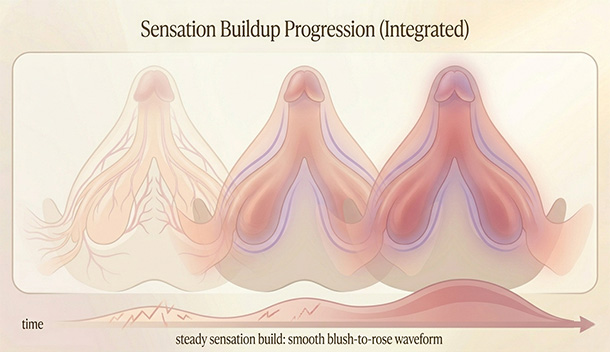
A sensation can be promising and still go nowhere if it keeps changing before your nervous system has had time to organize it into pleasure. Your body reads the signal, starts building, then has to stop and reread a new one. Start over. Adjust. Start over again. That’s exhausting, and it’s a big reason people end up saying they were close and then somehow lost it.
If that sounds familiar, you’re probably describing the same thing people mean when they get close to orgasm and then lose it. The build didn’t vanish for no reason. It got interrupted one too many times.
The moment people most often ruin it is the moment something starts to work
Something finally begins to feel good and the brain, in its infinite wisdom, decides now is the time to get ambitious.
So you speed up. Press harder. Move more directly onto the glans. Switch hands. Switch toys. Change the angle because maybe more intensity means you’re getting somewhere. Or you pause just long enough to check whether it’s working, which is often enough to knock yourself out of it.
That last one gets people all the time, especially if sex has started feeling like a performance review.
When you move from feeling the sensation to monitoring the sensation, attention changes jobs. The body can keep building while you’re inside the experience. It has a harder time when you’re hovering over it with a clipboard. That’s why performance pressure can kill pleasure even when the physical touch itself was perfectly decent.
When something starts working, the smarter move is usually boring: change less. Stay in the same lane longer than feels elegant. Give the sensation time to stack.
You don’t keep opening the oven because the bread finally started smelling good.
What this looks like in real life, with fingers, a vibrator, or a partner
Here is the plain version.
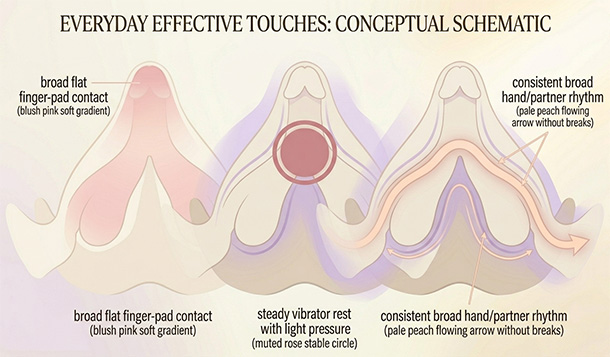
With fingers: flatter contact usually works better than people expect. Not the fingertip hunting for a target. More often it’s the pad of a finger, or two lubricated fingers, with enough lube that you’re gliding instead of dragging. The shift you’re looking for isn’t dramatic intensity. It’s the moment the touch stops feeling scratchy, too exposed, or weirdly hard to follow. If direct contact keeps feeling wrong, start a little wider and a little less bravely. That’s often where people find out what to try first when direct touch doesn’t feel good.
With a vibrator: the setting that works is often lower than the one that seems like it should work. Start two steps below your instinct and stay there longer than feels productive. Placement matters more than drama. For some people, the toy works best slightly off the most sensitive point, resting there with a light hand and very little movement. If a vibrator works better than fingers, that doesn’t mean your body is spoiled or numb or secretly broken. It usually means the device is delivering consistency your hand isn’t.
With a partner: the biggest upgrade is often less improvisation. A partner does one useful thing for four seconds, then changes it because they think they should escalate. Or they keep checking in so often that the body never gets to sink into the sensation. Good partner touch often has a very unglamorous quality to it. It listens longer than it performs. Sometimes the sexiest thing a hand can do is hold a working pattern for another sixty seconds and resist the urge to become an artist.
There are times when this really isn’t a technique issue
Sometimes the problem is the touch. Sometimes it’s the context. Sometimes your body has changed, and no amount of better angles is going to explain that away.
Orgasm difficulty can be shaped by medications, pelvic pain, hormonal shifts, dryness, menopause, mental health changes, surgery, chronic stress, and medical conditions that affect sensation or arousal. The same body can also respond differently from one week to the next. Tuesday’s touch can feel great. Thursday’s can feel like static. That isn’t inconsistency in the moral sense. It’s a nervous system responding to everything else that’s going on.
Slow down and talk to a clinician if you notice:
- new pain, burning, or soreness with clitoral touch
- a sudden drop in sensation, arousal, or orgasm ability
- changes that showed up after starting a medication, especially antidepressants or antihistamines
- distressing shifts around menopause, vaginal dryness, pelvic pain, or after gynecologic surgery
Mayo Clinic treats distressing orgasm difficulties as clinically relevant, which is useful because too many people wait until they’re miserable enough to justify asking for help. You don’t need to do that. A gynecologist, pelvic floor physical therapist, or sexual medicine specialist may be a much better use of your energy than another month of pressing harder and hoping for revelation.
The better question isn’t “what am I supposed to feel?”
That question sounds sensible, but it sends people chasing a universal sensation instead of paying attention to the one their own body is actually offering.
A better question is: what kind of touch does your body want to keep following?
That’s where the useful information lives. The contact that feels easier to stay with. The rhythm your body can recognize on the next pass. The kind of stimulation that doesn’t make you immediately start negotiating with it. Earlier I said you’re not looking for one perfect pixel, and this is the practical version of that idea. You’re learning the conditions under which sensation can gather instead of scatter.
Once you start reading your body that way, the whole thing gets less moral and more mechanical in the best sense. Less “why am I bad at this,” more “what signal can my nervous system actually use.” That shift tends to soften a lot of shame on its own.
Some bodies answer fast. Some need steadier contact, more buffering, less interference, fewer dumb cultural scripts in the room. None of that is especially glamorous. It is useful, though. And useful usually gets you further than sexy advice ever did.
Reviewed medical and clinical sources
- Cleveland Clinic. Clitoris: Anatomy, Location, Purpose & Conditions. Cleveland Clinic.
- Cleveland Clinic. Sexual Response Cycle: Order, Phases & What To Know. Cleveland Clinic.
- Mayo Clinic Staff. Anorgasmia in women: Symptoms and causes. Mayo Clinic.
- Mayo Clinic Staff. Anorgasmia in women: Diagnosis and treatment. Mayo Clinic.
- Department of Medical Psychology. Female Orgasmic Difficulties. Leicestershire Partnership NHS Trust.
Add comment