
You go to the place everyone says should feel best, and your body flinches.
Not because you are scared. Not because you are doing it wrong. Because the sensation itself feels too exposed. Too bright. Too close to the nerve.
For some people, direct touch does not feel sexy at first. It feels unshielded.
When I hear that, I do not think, you need more effort. I think, you need a different entry point. Cleveland Clinic’s clitoris anatomy guidance notes that the glans is extremely sensitive and that too much direct pressure can feel painful, while NHS guidance on female orgasmic difficulties notes that many women need steady clitoral stimulation, but that stimulation does not have to come from one exact kind of contact.
Start one layer away
If direct fingertip contact feels bad, do not make your first fix “try harder.”
Move one layer out.
For a lot of people, that small shift is the whole difference between contact that feels abrupt and contact that feels usable. The same area is still involved, but it starts landing more like indirect rather than fully direct clitoral stimulation.
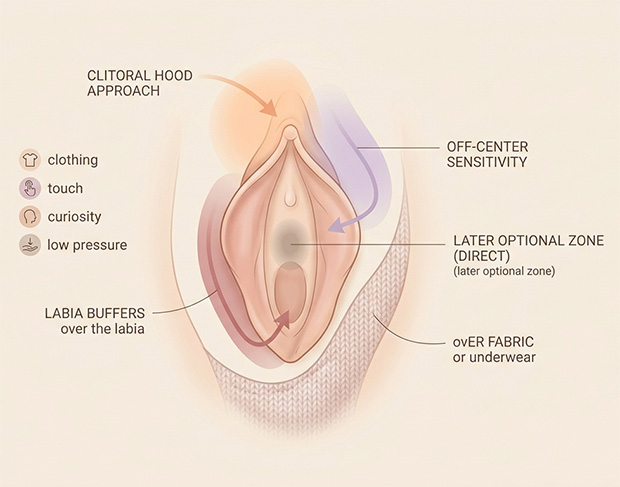
That might mean touching over the clitoral hood. It might mean touching just to one side. It might mean contact through underwear, sleep shorts, a thin sheet, or the flat pad of your finger instead of the tip.
It does not feel too light. It feels too naked.
That distinction matters. A lot of people abandon pleasure too early because they assume less-direct contact is a compromise. Often it is the thing that makes sensation usable. There is no prize for touching the most exposed part first.
I would start with one simple rule: do not aim straight for the center on the first pass. Approach from nearby tissue, stay there for a minute, and let your body decide whether it wants more.
Change the shape of the touch before the intensity
When direct touch feels bad, most people change pressure first.
I would change shape first.
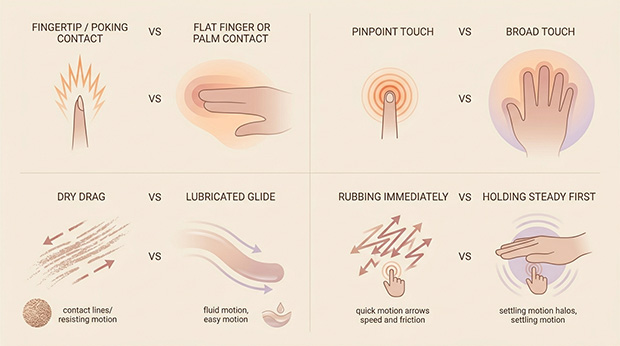
A poking fingertip can feel tiny and sharp. The flatter part of two fingers can feel wider and steadier. A small folded washcloth, a palm heel, or the side of a finger can turn contact from pinpoint to spread-out. Sometimes that is the whole shift.
For some bodies, the clitoris likes to be approached sideways.
Try contact that is flatter, broader, and more still. Then add movement only if the stillness starts to build into pleasure. Many people keep chasing sensation with quick rubbing when what their body wanted was a slower, buffered hold.
Broad touch can feel less like being struck and more like being held.
That is often the moment people realize the issue was never “not enough stimulation.” It was that the sensation was arriving too narrowly to build on, which is usually the deeper difference between broad and pinpoint clit stimulation.
Do not test direct touch before your body is there
This is the piece people skip because it sounds less technical than it is.
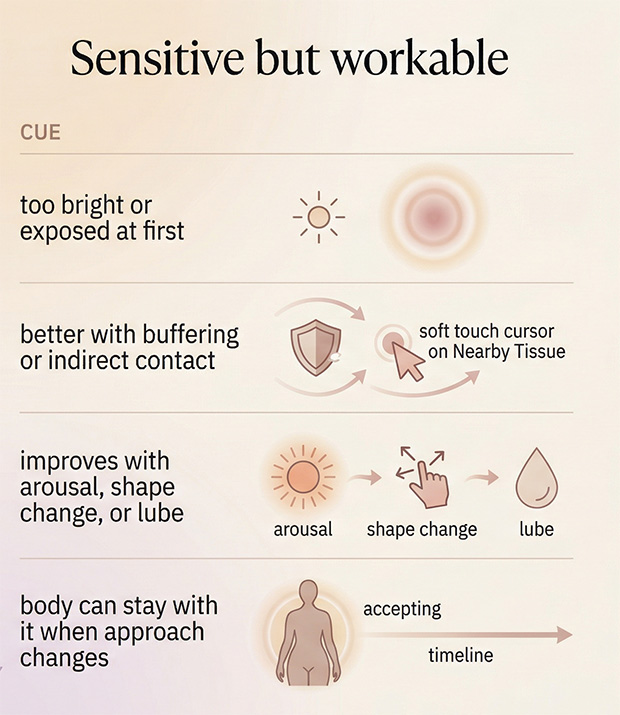
A lot of contact feels bad simply because it is early.
NHS guidance on vaginal dryness notes that discomfort can happen when you are not aroused yet, and that dryness can also be linked to menopause, breastfeeding, pregnancy, some medications, and hormonal shifts. That matters because what feels like “I hate touch” is sometimes “I hate friction before my body is ready for it.”
So before you try direct clitoral contact again, build arousal somewhere else first.
I would start with anything that makes your body feel more inhabited: thighs, breasts, stomach, inner hips, kissing, fantasy, pressure between the legs, a toy over fabric, or just rocking your hips against a pillow. You are not delaying the real thing. You are creating the conditions that let the real thing register as pleasure instead of static.
Sometimes the same touch that feels irritating at minute one feels welcome at minute eight.
That is not inconsistency. That is arousal.
For a lot of bodies, direct touch does not become readable until arousal has already spread through the rest of the system. That is usually the missing piece when it helps to build arousal before bringing in more targeted stimulation.
Use glide before you use more stimulation
A surprising amount of “I do not like this” is really “I do not like this much drag.”
Dry touch can feel scratchy. It can skip. It can catch on the skin. Even when you are focused on external touch, lubrication can change the entire quality of sensation.
NHS advice on vaginal dryness recommends water-based lubricants before sex, including on fingers and sex toys, and ACOG’s patient guidance on painful sex notes that water-soluble lubricants are a good choice when irritation or sensitivity is part of the picture.
I use lube here as a sensation tool, not just a pain-prevention tool.
It can make the difference between friction and glide. Between rubbing and floating. Between “too much” and “oh, that’s better.”
If direct touch feels harsh, add a small amount of lube and try the same buffered contact again before you decide the method does not work.
What this looks like in real life
This gets easier when you can picture it.
- If your first instinct is to pull your hand away after two seconds: start over clothing or underwear, use the flat part of two fingers, and stay off the center. Hold steady. Do not rub right away.
- If it only starts to feel good much later: stop treating the first minute as the test. Spend five to ten minutes building arousal elsewhere, then return with broader contact and more glide.
- If a toy feels better than fingers: that does not mean your body is “dependent” on toys. It may mean the toy gives steadier, more even stimulation than a fingertip does. NHS orgasm guidance explicitly notes that many women reach orgasm more reliably from fingers, oral stimulation, or vibrators than from intercourse alone.
- If you like pressure but not rubbing: try grinding against a pillow, folded blanket, or your own hand instead of stroking the area directly. Some bodies prefer pressure that builds through the surrounding tissue.
That last one matters more than people think.
Some people do not want the clitoris touched so much as activated.
For some bodies, the better entry point is pressure through surrounding tissue rather than direct rubbing on the most exposed part. That is often the practical difference between different ways pleasure builds even when the same general area is involved.
A five-minute reset if direct touch keeps failing
If I wanted a reader to try one thing tonight, it would be this:
- Spend one minute touching anywhere except the most sensitive spot.
- Add a little lube.
- Use broad contact over the hood, labia, or fabric for another minute.
- Keep the pressure steady before adding motion.
- Only then test a little closer, and back off the second it turns sharp.
Not because you are being cautious.
Because you are getting better information.
The body usually tells the truth faster when it is not defending itself.
When “sensitive” is actually pain
There is also a line I would not ignore.
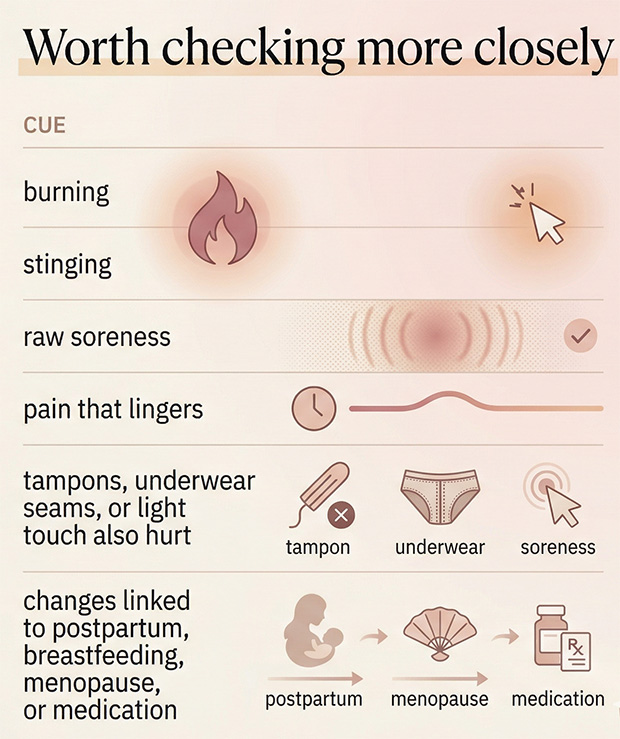
If the sensation is not merely intense but burning, stinging, raw, or sore in a way that lingers, this may be more than a preference issue. NHS guidance on vulvodynia describes vulvar pain that can start when the vulva is touched and may feel like burning or stinging, and Cleveland Clinic notes that hypertonic pelvic floor can also show up as pain with sex and difficulty with orgasm because the muscles are not relaxing well.
I would pay attention if any of this sounds familiar:
- Light touch feels painful, not just intense.
- Tampons, penetration, or even a seam in underwear can feel sharply uncomfortable.
- You notice burning, stinging, or soreness that hangs around after sexual touch.
- The problem showed up with dryness, postpartum changes, breastfeeding, menopause, or a medication change.
That is where “keep experimenting” stops being useful advice on its own.
NHS guidance says persistent vulvar pain deserves assessment, and notes that clinicians may examine the area gently and rule out infections or skin conditions. Cleveland Clinic’s pelvic floor guidance also points to pelvic floor physical therapy as a main treatment when muscle over-tightening is part of the problem.
So if direct touch never feels good, or has recently become painful, I would not treat that as a personal quirk you are supposed to silently work around forever.
The better question
A lot of people ask, “Why can’t I handle direct touch?”
I think the better question is, “What kind of contact can my body actually receive?”
That changes everything.
It moves you out of the mindset where pleasure is a test of tolerance, and into one where pleasure is a matching problem. Texture, angle, timing, pressure, arousal, friction, muscle tension, hormones. Those are not excuses. They are the map.
Pleasure is not a bravery test.
That shift matters because a body that keeps bracing against contact is not asking for more courage. Very often, it is asking for less guarding and a different kind of contact.
The right first move is the one your nervous system does not have to fight.
Reviewed medical and clinical sources
- Cleveland Clinic. “Clitoris: Anatomy, Location, Purpose & Conditions.” Cleveland Clinic.
- Leicestershire Partnership NHS Trust, Department of Medical Psychology. “Female Orgasmic Difficulties.” NHS.
- NHS. “Vaginal Dryness.” NHS.
- NHS. “Vulvodynia (Vulval Pain).” NHS.
- Cleveland Clinic. “Hypertonic Pelvic Floor: Symptoms, Causes & Treatment.” Cleveland Clinic.
- American College of Obstetricians and Gynecologists (ACOG). “When Sex Is Painful.” ACOG.
Add comment