
You bring in a vibrator because your hand alone is not quite enough. Or you add fingers because the vibrator feels good but somehow too flat, too sharp, too disconnected. Then the moment you try both together, everything gets messier. You lose the spot. The rhythm breaks. What was working suddenly is not.
That does not mean your body is complicated in some broken way.
Usually it means too many things are happening without enough structure.
I want to make one distinction early. Combining fingers and a vibrator is not automatically about making stimulation stronger. For a lot of people, it works because it makes stimulation more precise, more supported, or more layered. Mayo Clinic notes that many women need direct manual or oral clitoral stimulation because penetration alone may not be enough for orgasm, and an NHS psychosexual leaflet makes a similar point: many women need steady clitoral stimulation, often from fingers or a vibrator rather than intercourse alone.
Start with a division of labor, not two things doing the same job
The best finger-and-vibrator combo does not feel busier.
It feels more organized.
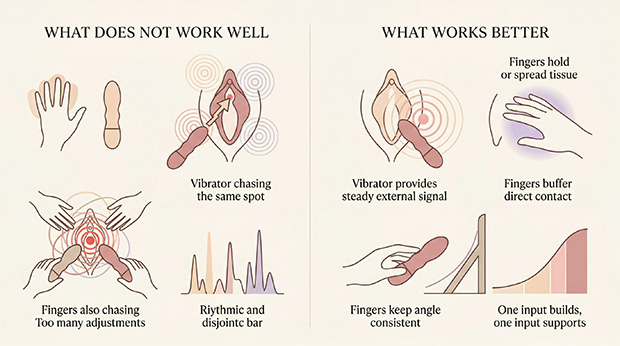
Most failed attempts go wrong for one reason: both inputs are trying to do the exact same thing. The vibrator is hunting the clitoris. Your fingers are also hunting the clitoris. Both are moving. Both are adjusting. Both keep interrupting each other.
That usually creates scatter instead of build.
I get much better results when I think in roles. One part creates the sensation. The other part protects it.
Good role splits often look like this:
- the vibrator provides steady external stimulation while fingers spread or hold tissue in place
- the vibrator stays still while a finger adds gentle internal fullness
- a finger acts as a soft buffer while the vibrator works through it
- fingers keep the angle consistent so the toy does not skid off every few seconds
That logic lines up with what good clinical guidance says about orgasm difficulty: the type of stimulation matters, the amount of stimulation matters, and some orgasm problems are situational rather than universal. Mayo Clinic’s overview of anorgasmia and the Merck Manual’s overview of female orgasmic disorder both describe orgasm response as something that depends on the specific kind of stimulation and context, not just desire or effort.
Your fingers can change the shape of sensation, not just add more of it
A lot of people treat fingers as a second stimulation source when they are often more useful as a positioning tool.
That matters.
Sometimes the breakthrough is not stronger contact. It is better contact.
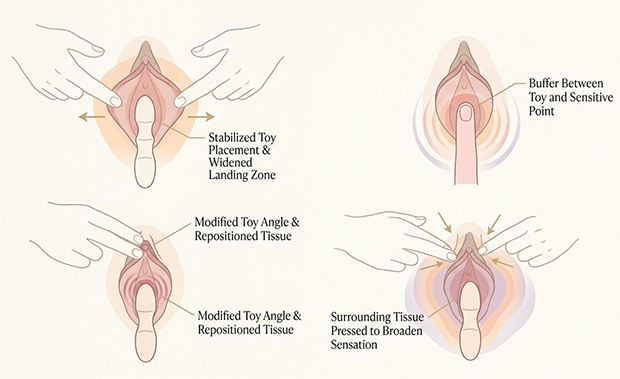
Your fingers can pull the outer labia slightly apart so the vibrator stops slipping. They can flatten or lift the clitoral hood a little, which can make the same toy feel either more direct or more cushioned. They can press the surrounding tissue above the clitoris so the sensation feels broader and less thin. They can also rest between the toy and your most sensitive spot, which softens the edges without removing the vibration entirely.
It does not feel smaller.
It feels less thin.
For a lot of people, that is the whole improvement. The sensation is still clearly clitoral, but it lands with a little more cushion and spread, which is often the deeper difference between direct and indirect clitoral stimulation.
This is one reason anatomy matters here. The clitoris is not just the visible glans. As Cleveland Clinic’s anatomy overview explains, it is a larger structure with parts inside and outside the body. That helps explain why changing tension, pressure, or tissue position with your fingers can change how external vibration lands, even when the toy itself has not changed.
There is also a very practical issue people underestimate: drag. Once you add both fingers and a toy, friction starts mattering more. MedlinePlus guidance on sexual pain specifically recommends more arousal before penetration and using lubricant for dryness, and that applies here too. A little glide can be the difference between “nothing is building” and “oh, there it is.”
If you want internal and external stimulation together, keep one of them simple
This is where people often overdo it.
They insert fingers and start curling. The vibrator is moving too. Pressure changes every second. The body has no stable signal to organize around.
If you want to combine internal fingers with an external vibrator, start by making one of them boring. I mean that in the best possible way.
Let the vibrator do the active work and keep one finger inside mostly still. Not stiff. Just steady. Think light upward pressure, fullness, or presence. Then notice what changes. For some bodies, that added fullness makes external stimulation feel more anchored and more whole.
When that happens, the useful shift is not that everything got stronger. It is that the body suddenly has more than one line of sensation to organize at once, which is often what people are trying to describe when blended stimulation feels fuller and easier to build on.
Because the clitoris includes internal erectile structures, some people experience internal-plus-external stimulation as more layered rather than merely stronger. At the same time, penetration by itself often does not provide enough clitoral input for orgasm, which is exactly why this combination can work so differently from penetration alone. Cleveland Clinic, Mayo Clinic, and the NHS psychosexual leaflet all support those two parts of the picture.
What usually works worst is trying to make both sensations equally dominant from the start.
Do not make both inputs compete for your attention at the same moment.
Add the second input later, not sooner
A lot of people bring in the second input too early.
They start from zero with toy plus fingers plus movement plus angle changes, then wonder why it feels mechanical. But arousal usually builds from continuity, not from complexity.
Pleasure often drops not because you lost arousal, but because you lost continuity.
That is often the exact moment a good combination starts failing. The body was locking onto something useful, and then the added input broke the line of it, which is the same reason people get close to orgasm and then lose it when too much changes at once.
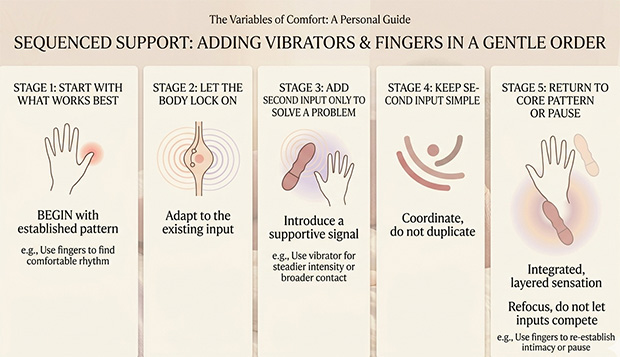
I usually suggest starting with the thing that already works best for your body. Let that build for a minute or five. Once you feel your body locking onto the pattern, then bring in the second input carefully. Not as a surprise. As support.
That approach fits clinical guidance on orgasm difficulty. Mayo Clinic’s diagnostic questions specifically distinguish between activities, partners, and situations, which is a good reminder that your body may not need a bigger technique. It may just need the right sequence.
So if the combo has never worked, try this instead:
Start with fingers alone if your body likes warm, responsive, skin-on-skin buildup. Add the vibrator only when you want steadier intensity.
Or start with the vibrator alone if consistency helps you get close. Add fingers only when you need more support, a softer buffer, or internal fullness.
The second input should solve a problem.
It should not create a new one.
What this looks like in real life
When the toy feels good, but you keep losing the spot
This is common with small bullets and curved suction-style toys.
Use two fingers of your non-dominant hand to gently separate or steady the outer tissue. Do not actively rub with those fingers. Just hold the area open and quiet. Then let the toy do the work. A lot of people find that what felt slippery and inconsistent suddenly becomes much easier to follow.
You are not adding stimulation there.
You are removing noise.
When direct vibration gets intense too fast
Put a finger or two between the toy and the most sensitive point, or use your fingers to pull the contact slightly higher, lower, or to one side. The vibrator still comes through, but the sensation spreads out. This can feel dramatically better for people who do not want the clitoral glans hit head-on every second. That is also consistent with mainstream medical guidance noting that many people need clitoral stimulation, but not always in the same exact form or directness every time.
When you want more fullness without losing external pleasure
Insert one lubricated finger and leave it there with light pressure rather than active thrusting. Then place the vibrator where external stimulation already feels best. If that feels good, you can later add a tiny internal curl or pulse. But earn that complexity. Do not begin there.
For many people, the useful difference is simple: the finger gives context, and the vibrator gives signal.
When the combo keeps failing, the issue may not be technique at all
Sometimes fingers plus a vibrator feels bad because the technique is off.
Sometimes it feels bad because your body is protecting you.
When that is the layer underneath the problem, better coordination will only get you so far. Sometimes the real issue is that the body is too guarded for pleasure to build cleanly, no matter how clever the technique is.
If adding fingers causes burning, stinging, sharp entry pain, or that immediate involuntary “nope” feeling where the muscles close down before you even mean them to, do not treat that like a coordination problem. NHS guidance on vaginismus describes exactly that kind of automatic tightening, and it can happen even in people who still feel desire and enjoy external pleasure.
Likewise, if sex or insertion has become newly painful, suddenly dry, or hard to enjoy, do not just increase vibration and hope to overpower it. MedlinePlus advises seeking care when pain with sex is distressing or suddenly appears, and Mayo Clinic notes that dryness, vaginismus, medications such as SSRIs, menopause-related changes, and other medical factors can all affect orgasm and comfort.
That matters because no technique article should quietly teach people to push through pain.
If the combo keeps failing in a way that feels defensive rather than neutral, step back. Use more lubrication. Return to external-only play if that still feels good. And if pain, numbness, or a sharp change in orgasm response keeps showing up, talk to a clinician who takes sexual pain and orgasm concerns seriously.
The point is not to do more.
It is to stop asking one small area to do every job at once.
When fingers and a vibrator work well together, the sensation usually does not feel crowded. It feels supported. One part builds. One part guides. One part steadies what would otherwise get lost.
That is the real shift.
Not more stimulation. Better architecture.
Reviewed medical and clinical sources
- Mayo Clinic Staff. “Anorgasmia in women – Symptoms and causes.” Mayo Clinic, February 29, 2024. Read source
- Mayo Clinic Staff. “Anorgasmia in women – Diagnosis and treatment.” Mayo Clinic, February 29, 2024. Read source
- “Clitoris: Anatomy, Location, Purpose & Conditions.” Cleveland Clinic, updated January 26, 2026. Read source
- “Orgasmic dysfunction in women.” MedlinePlus Medical Encyclopedia, reviewed April 16, 2024. Read source
- “Women and sexual problems.” MedlinePlus Medical Encyclopedia, review date November 8, 2024. Read source
- “Vaginismus.” NHS. Read source
- Department of Medical Psychology. “Female orgasmic difficulties.” Leicestershire Partnership NHS Trust. Read source
- “Female Orgasmic Disorder – Gynecology and Obstetrics.” Merck Manual Professional Edition. Read source
Add comment