
You can make yourself come. You know your body works.
Then you are with someone else, and suddenly everything gets harder in a way that makes no sense from the outside. You get close. A hand shifts. The pace changes. They ask, “Like that?” You leave your body for half a second to answer, and the whole thing thins out.
It is one of the most confusing sexual experiences there is.
It does not feel like failure exactly. It feels like losing the thread.
If you orgasm alone, the real question changes
If you can orgasm alone, the question usually is not whether your body is capable of orgasm. It is what conditions your body needs, and what changes when another person enters the room.
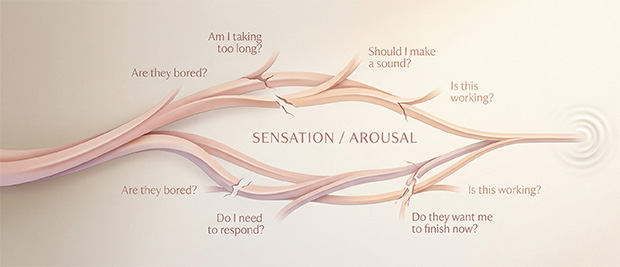
That distinction matters more than people think. Female orgasm depends on mind and body working together, and a lot can interfere with that when sex becomes shared instead of private: anxiety, divided attention, embarrassment about asking for the touch that actually works, worrying about whether you are taking too long, worrying about whether your partner is bored, worrying about whether you are making the right noises so they know it is going well. None of that is exotic. It is just extra traffic in the same nervous system that is trying to stay inside sensation.
There is also a blunt mechanical reason partnered sex often feels less reliable than solo sex. In large U.S. survey data, intercourse alone was enough for orgasm for a minority of women. Many said clitoral stimulation was necessary during intercourse, and many more said orgasm felt better when it was added. Other research found the same pattern from a slightly different angle: orgasm reports were higher during intercourse that included clitoral stimulation and lower during unassisted intercourse.
So if you orgasm alone but not with a partner, that is not a contradiction.
It is a clue.
Partnered sex changes a lot more than the source of touch
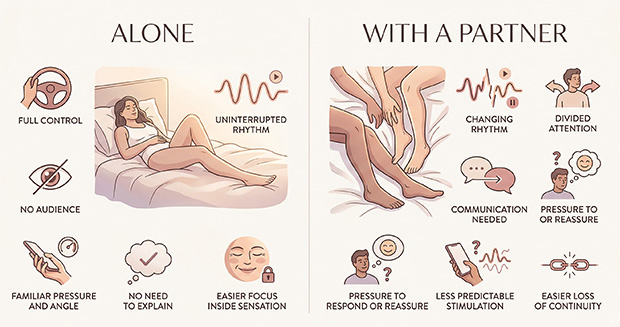
When you are alone, you do not have to be readable.
You do not have to reassure anyone, perform arousal clearly enough to be understood, or manage another person’s feelings in real time. You do not have to think about whether they are silently waiting for the “big moment.” You do not have to decide whether now is a good time to say, no, actually, go a little higher and slower and please do not improvise.
That is a lot to hold while trying to follow pleasure.
NHS psychosexual guidance points out that pressure to orgasm for a partner can itself make orgasm harder. That tracks. Plenty of people can stay deep inside sensation right up until they feel observed from the outside. The body can still be turned on. It just gets much harder to follow the feeling once orgasm starts competing with distraction instead of being allowed to take over.
This is why partnered orgasm can fall apart even with someone kind, attractive, and genuinely invested. The problem is often not lack of desire.
It is divided attention.
Orgasm usually depends on continuity, and partnered sex keeps breaking it
A lot of people think orgasm is mostly about intensity. More pressure. More speed. More enthusiasm. More effort.
Often it is much more about continuity.
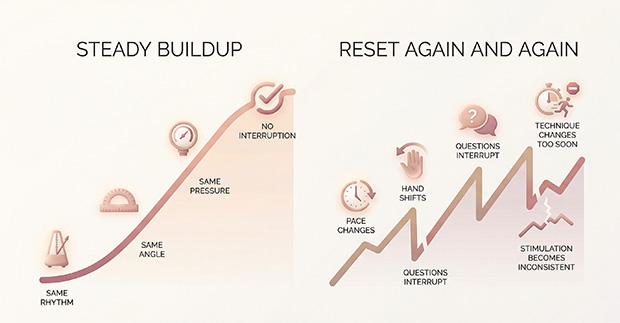
When you are alone, nobody interrupts the sentence your body is writing. You keep the same angle. The same pressure. The same pace. You do not switch techniques because you got excited and decided to “mix it up.” You do not stop to check whether it is happening yet. You do not move the touch three millimeters left right when it was finally starting to work.
A partner can be loving and still be rhythmically wrong.
That is not an insult. It is just reality. A buildup that might have tipped into orgasm alone keeps getting reset in partnered sex because the rhythm changes, the pressure drifts, the check-ins pull you into language, or the touch gets more dramatic at exactly the wrong moment. That is often what people are naming when they say they were almost there and then suddenly not there at all. The build did not necessarily fail. It got interrupted in the same way people get close to orgasm and then lose it.
Again and again.
Your solo method is probably more specific than you realize
Most people do not orgasm from a generic category of touch.
They orgasm from a very particular version of that touch. Not “clitoral stimulation.” A certain side. A certain firmness. A certain amount of glide or drag. A certain rhythm that seems almost boring until it suddenly is not. Maybe there is thigh tension involved. Maybe a held breath. Maybe a tiny pelvic rock. Maybe a slowdown right before the edge, then a return to the original pace.
Large survey data on women’s genital touch found wide variation not only in whether clitoral stimulation helped, but in preferred location, pressure, shape, and pattern. That matters here, because “do what I like” sounds simple until you realize what you like may be extremely precise.
That is one reason solo orgasm does not automatically transfer to partnered sex. Your hand already knows the pressure before you consciously name it. Your body adjusts in tiny ways without discussion. You are not just touching yourself. You are running a familiar sequence.
With a partner, all that invisible knowledge has to be translated.
And translation is where a lot of people lose the plot.
What this looks like in real life
Sometimes it looks like this:
You are aroused. They are touching the right area. But their hand keeps drifting wider when your body wanted narrower.
Or they are doing exactly what you asked, but they keep checking whether it is good, and every check-in pulls you an inch out of the moment.
Or you can feel orgasm building, but the second they notice, they speed up dramatically, as if enthusiasm will finish the job. It does not. It scrambles the pattern.
Or penetration is happening, and everybody is treating that as the main event while the kind of clitoral contact you usually need is absent, inconsistent, or too indirect to keep the buildup alive. Research on orgasm during intercourse shows why this matters: women report orgasm much more often when clitoral stimulation is part of the picture than when intercourse is unassisted.
One of the roughest versions is this: you are close, you know you are close, and then you become aware that your partner is waiting for you to be close.
That awareness alone can be enough to break it.
A lot of bodies can stay inside pleasure right up until they start feeling observed from the outside. Once that happens, performance pressure can get louder than sensation, even when nobody meant to create it.
What actually helps without turning sex into a performance review
I would treat your solo orgasm as data, not as some separate category of sex that does not count.
That is the map.
What usually helps is not “trying harder together.” It is protecting the conditions that already work and bringing them into partnered sex more honestly. Guidance on orgasm problems includes focusing on sexual activities beyond intercourse, being more explicit about what kind of touch works, and using clitoral stimulation or a vibrator when helpful. None of that is cheating. It is basic problem-solving.

A few changes usually matter more than grand emotional speeches:
- Get more specific than body-part names. “Up a little, firmer, don’t circle, stay there” is much more useful than “touch my clit.”
- Protect the last minute before orgasm. If changes usually ruin it, say that before sex starts, not when you are already trying not to lose the thread.
- Let your own hand or a toy stay in the mix. For some people, the easiest way to preserve continuity is keeping one familiar source of touch while the other adds around it, which is often how fingers and a vibrator work well together instead of pulling the body in two directions.
- And take orgasm off the job description for a few sessions. Less audience, more sensation.
The goal is not to make partnered sex identical to solo sex.
It is to stop partnered sex from constantly interrupting what your body already knows how to do.
Sometimes this stops being a technique issue
Sometimes this really is about context, timing, attention, and stimulation. Sometimes it is not.
If orgasm became harder after starting an SSRI or another medication, during perimenopause or menopause, after the onset of pelvic pain, with vaginal dryness, after trauma, or alongside a condition that can affect nerves or blood flow, that deserves more than bedroom troubleshooting. Medication effects, hormonal changes, chronic pelvic pain, vaginismus, multiple sclerosis, diabetes-related nerve changes, and other medical factors can all affect orgasm.
The same goes if the shift is sudden, persistent, distressing, or happening across the board rather than only with one partner or in one type of situation. Clinical definitions of orgasm disorder are not based on one bad night. They are based on a pattern over time and the distress it causes.
That is the point where I would stop blaming chemistry, stop blaming myself, and talk to a clinician or a qualified psychosexual therapist.
Because sometimes the body is asking for better technique.
And sometimes it is asking for care.
The lens I’d leave you with
If you can orgasm alone, your body is not withholding something from your partner out of spite. It is not broken in private and broken differently in public.
It is already communicating.
Solo orgasm is not cheating. It is not lesser. It is not evidence that you are bad at sex with another person. It is evidence that, under the right conditions, your body gives clear information.
The work is not teaching your body how to orgasm with a partner from scratch.
The work is helping partnered sex stop drowning out the instructions.
Reviewed medical and clinical sources
- National Library of Medicine. Orgasmic dysfunction in women. MedlinePlus Medical Encyclopedia.
- National Library of Medicine. Women and sexual problems. MedlinePlus Medical Encyclopedia.
- Allison Conn, MD; Kelly R. Hodges, MD; reviewed by Oluwatosin Goje, MD, MSCR. Female Orgasmic Disorder. MSD Manual Professional Edition.
- University Hospitals Bristol and Weston NHS Foundation Trust. Psychosexual service: I’m having trouble achieving an orgasm (anorgasmia). NHS.
- Debby Herbenick, Tsung-Chieh Jane Fu, Jennifer Arter, Stephanie A. Sanders, Brian Dodge. Women’s Experiences With Genital Touching, Sexual Pleasure, and Orgasm: Results From a U.S. Probability Sample of Women Ages 18 to 94. Journal of Sex & Marital Therapy.
- Talia Shirazi, Kaytlin J. Renfro, Elisabeth Lloyd, Kim Wallen. Women’s Experience of Orgasm During Intercourse: Question Semantics Affect Women’s Reports and Men’s Estimates of Orgasm Occurrence. Archives of Sexual Behavior.
Add comment